Thumb basilar joint arthritis (also called thumb CMC arthritis) is wear and loss of cartilage in the joint at the base of the thumb. The joint carries enormous load during pinch and grip, and is one of the most common sites of hand arthritis. Typical symptoms are pain with pinching, opening jars, turning keys, and writing. Early treatment focuses on splinting, corticosteroid injection, and hand therapy. When pain persists or injections stop providing relief, Dr. Loredo performs joint reconstruction (most commonly trapeziectomy with ligament reconstruction and tendon interposition, or suture suspension arthroplasty) to restore comfortable thumb function.
The Anatomy of the Thumb CMC Joint
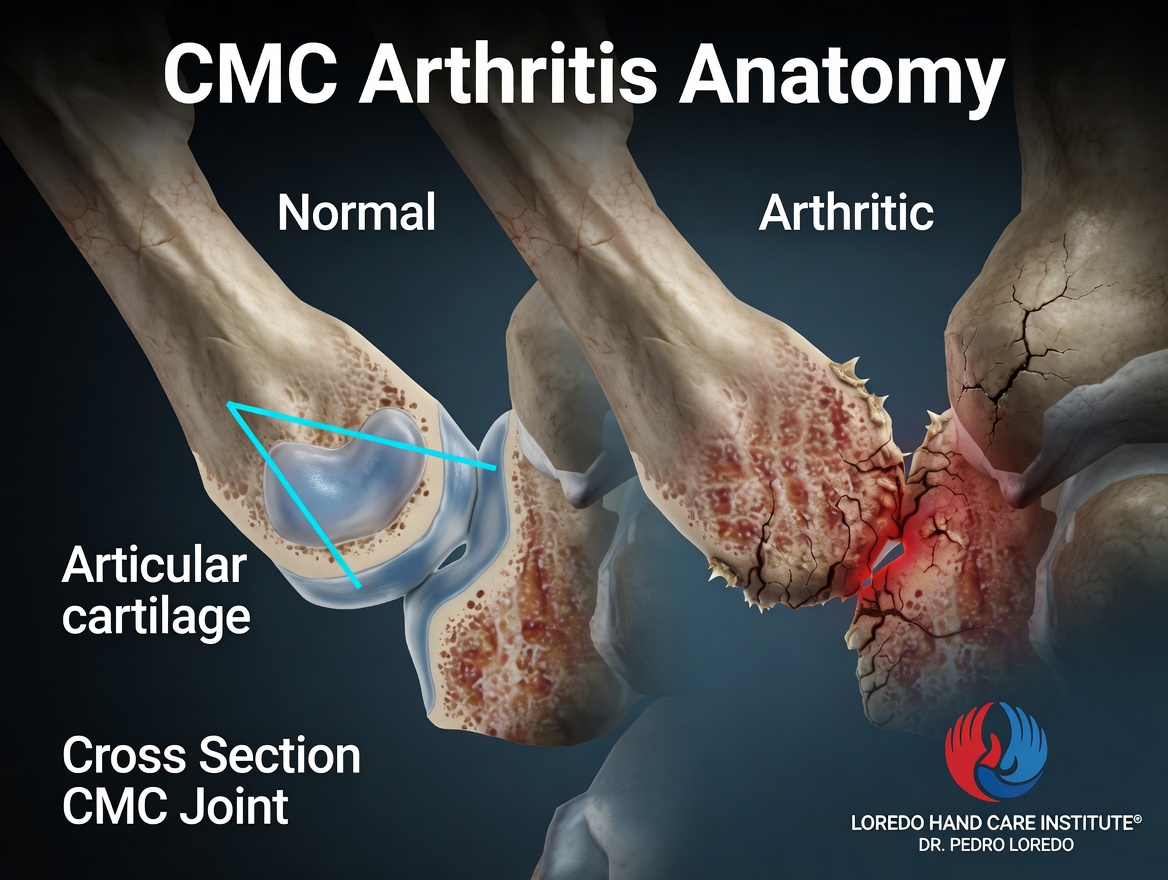
The thumb carpometacarpal (CMC) joint sits at the base of the thumb, where the thumb metacarpal meets the trapezium bone of the wrist. The joint has a saddle shape that allows the thumb to move in multiple planes: flexion and extension, abduction and adduction, and opposition to reach the other fingers. This mobility is essential for pinch, grip, and precision tasks. It also makes the joint the most heavily loaded joint in the hand. Cartilage loss over time leads to bone-on-bone contact, capsular laxity, progressive deformity, and the painful loss of thumb function we call basilar arthritis.
Thumb CMC arthritis affects women more often than men and typically presents after age 40.
Clinical coding: ICD-10 M18.9 (osteoarthritis of first carpometacarpal joint). SNOMED CT 203440008.
Causes and Risk Factors
- Age: cartilage wear accumulates with use; most commonly symptomatic after age 40
- Female sex: women are affected roughly six times more often than men
- Prior thumb injury: Bennett or Rolando fracture, ligament injuries, or prior dislocation accelerate joint wear
- Occupational or recreational thumb loading: sewing, manual trades, prolonged texting, and certain sports
- Generalized osteoarthritis: patients with other arthritis sites are more prone to CMC arthritis
- Family history
- Laxity of the beak ligament (anterior oblique ligament), which allows abnormal joint motion over time
Symptoms and Warning Signs
- Pain at the base of the thumb with pinching, gripping, or twisting a key or jar
- Pain that worsens with activities like writing, sewing, opening pill bottles, or turning a door handle
- Weakness of pinch and grip
- A swollen, tender bump at the base of the thumb
- Grinding, clicking, or a grating sensation with thumb motion
- Stiffness on first use in the morning that loosens with activity
- In advanced disease, a "shoulder sign" deformity: the thumb metacarpal drifts inward and the base of the thumb becomes more prominent
- Compensatory hyperextension of the thumb MCP joint as the CMC collapses
How the Diagnosis Is Made
Dr. Loredo performs a focused examination including the following tests:
- Grind test (CMC compression test): gentle axial compression of the thumb metacarpal with rotation reproduces pain and often a grinding sensation. The most sensitive bedside test.
- Palpation of the CMC joint line for tenderness and swelling.
- Volar subluxation assessment: the thumb metacarpal base can be shifted forward over the trapezium in advanced disease.
- Range of motion and pinch and grip strength measurement.
- Assessment of the thumb MCP joint for compensatory hyperextension.
Standard X-rays (anteroposterior and lateral thumb, plus a stress view) confirm the diagnosis and grade the severity using the Eaton-Littler or Eaton-Glickel classification. MRI is not typically required. Imaging of coexisting conditions (scaphotrapezial arthritis) may change the surgical plan.
Non-Surgical Treatment Options
- Custom thumb spica splinting for activity and night use. A well-fitting splint offloads the CMC joint and reduces pain. Short-opponens splints allow most daily tasks while protecting the joint.
- Oral medications. NSAIDs (ibuprofen, naproxen) reduce inflammation and pain at the CMC joint. Acetaminophen helps with pain relief. Topical anti-inflammatory creams provide localized relief without systemic effects. Dr. Loredo reviews medical history and current medications before recommending any prescription option.
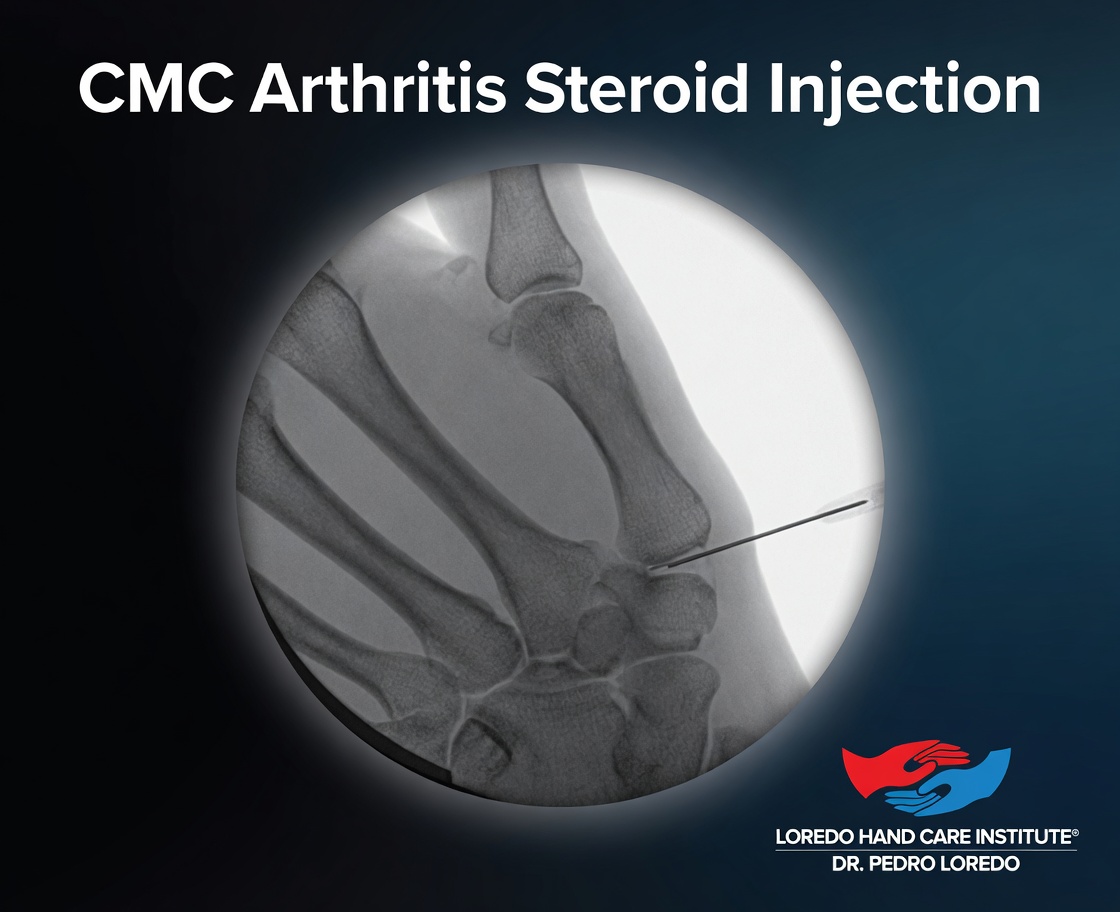
- Fluoroscopy-guided corticosteroid injection into the CMC joint. Image guidance ensures precise needle placement directly into the joint space, providing meaningful pain relief for many patients. Injections are repeatable periodically as effect wanes.
- Targeted hand therapy: first dorsal interosseous strengthening, thenar strengthening, and joint-protection education.
- Activity modification and ergonomic tools: built-up grips for utensils, jar openers, key turners, and modified pens reduce load on the joint.
Many patients manage thumb CMC arthritis for years with these measures. Surgery enters the conversation when conservative care no longer controls pain, when injections lose their effect, or when the joint limits activities you want to continue.


Surgical Options
All modern surgical treatments remove the worn-out trapezium bone and stabilize the thumb. The difference is how the thumb is supported after trapezium removal.
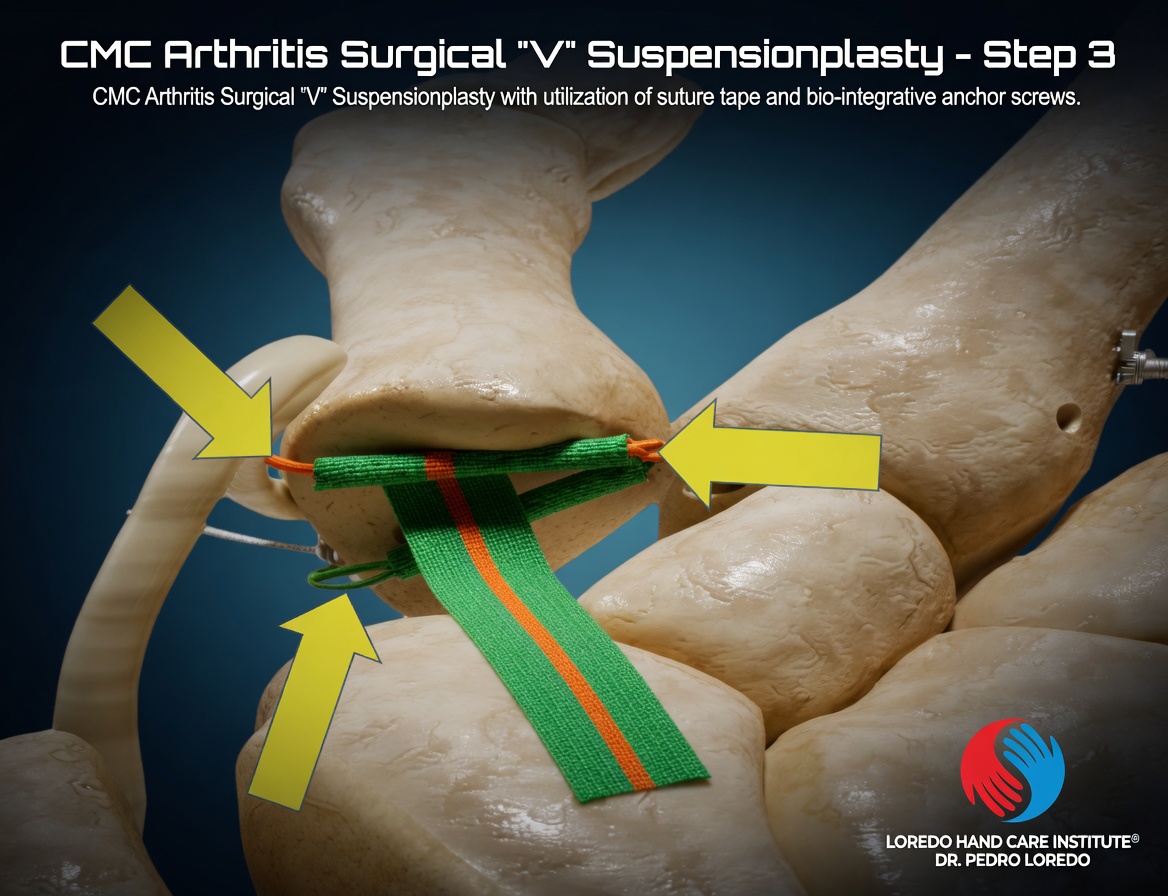
Suture Suspensionplasty with Bio-Integrative Anchor Screws (Dr. Loredo's primary surgical approach)
Dr. Loredo performs a modern V-configuration Suture Suspensionplasty using strong suture tape and bio-integrative anchor screws. This technique removes the arthritic trapezium and stabilizes the thumb metacarpal in proper position without sacrificing the FCR tendon. The bio-integrative anchor screws gradually integrate with the patient's own bone, while the suture tape provides immediate strength to the reconstruction.
- The arthritic trapezium is fully removed
- Bio-integrative anchor screws are placed in adjacent stable bone (typically the index finger metacarpal base and the thumb metacarpal base)
- High-strength suture tape is woven in a V-configuration between the anchors to suspend the thumb metacarpal in proper anatomic position
- No FCR tendon is harvested, preserving wrist flexor strength and avoiding the small donor-site morbidity of LRTI
- Bio-integrative anchors gradually convert to bone, leaving no permanent foreign material long term
- Faster return to hand use compared to traditional LRTI
- Excellent pain relief with durable functional outcomes
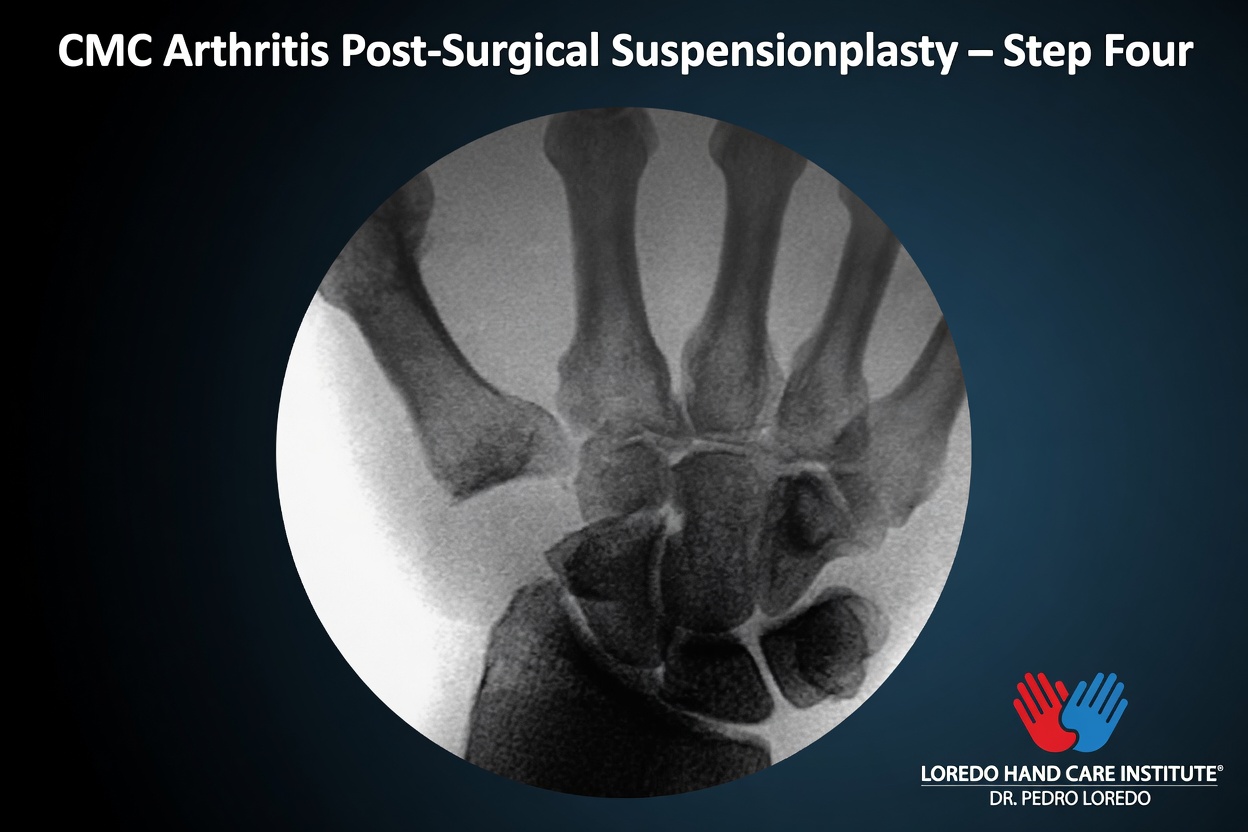
The Four Surgical Steps
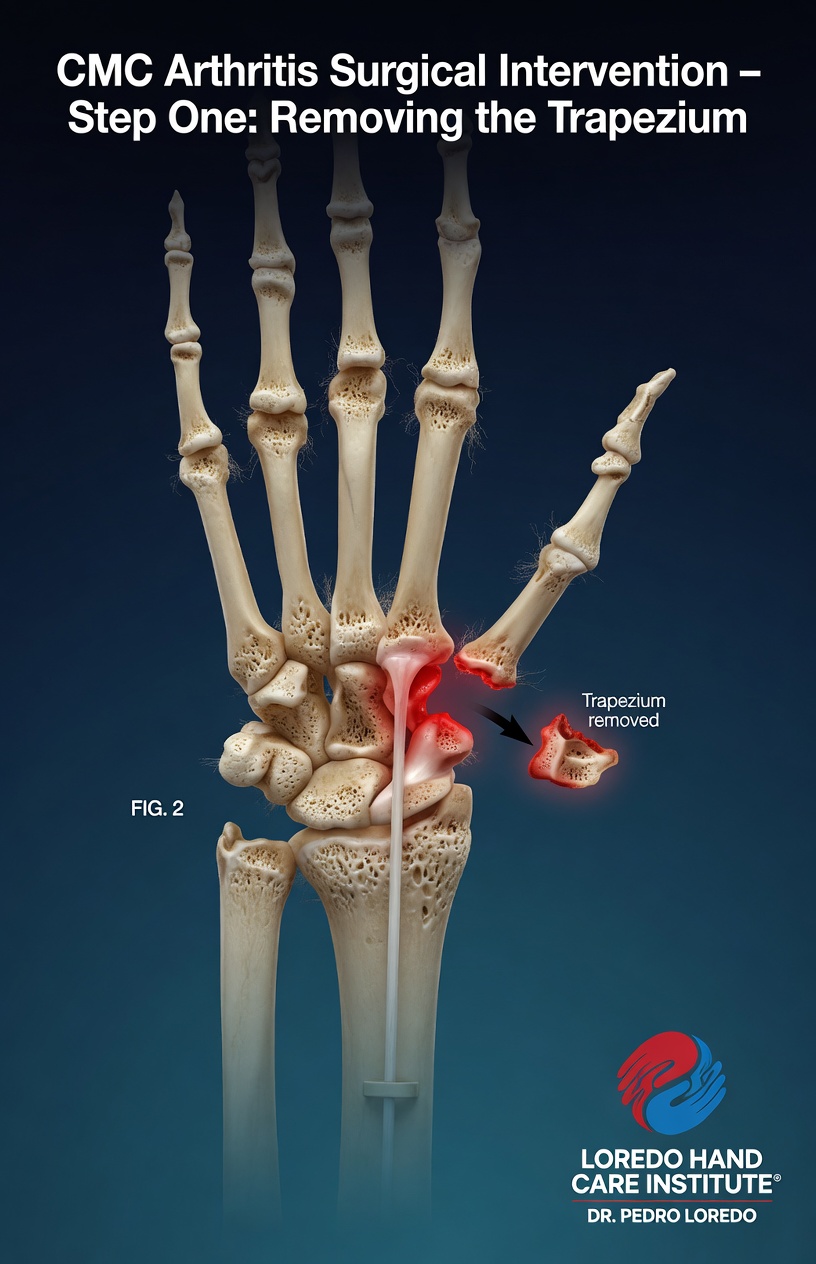

Trapeziectomy with Ligament Reconstruction and Tendon Interposition (LRTI)
- The traditional, most historically established procedure, with decades of good long-term outcomes
- The trapezium is removed
- A strip of the flexor carpi radialis (FCR) tendon is harvested, used to reconstruct the thumb's beak ligament, and rolled to fill the space the trapezium occupied
- Thumb is protected in a cast or splint for 4 to 6 weeks
- Excellent pain relief and durable functional outcomes
- Considered as an alternative when patient anatomy or specific clinical factors favor the tendon-based reconstruction
Joint-Specific Reconstructions
Trapezial implant arthroplasty, partial trapeziectomy with interposition, and arthroscopic debridement have specific indications. These are considered on a case-by-case basis for younger patients or early-stage disease.
Recovery Timeline
- Day 0: Outpatient surgery under regional block and sedation. A thumb-protecting splint or cast is applied.
- Week 1 to 2: First follow-up visit. Dressing changed. Gentle finger motion allowed; the thumb is protected.
- Week 2 to 4: Continued thumb immobilization. Fingers, wrist, and elbow move freely.
- Week 4 to 6: Transition to a removable thumb splint. Hand therapy begins for gentle thumb motion and light pinch.
- Week 6 to 12: Progressive strengthening under hand therapist guidance. Return to most daily tasks.
- Month 3 to 6: Full return to most activities. Strength continues to improve.
- Month 6 to 12: Continued strength gains and scar remodeling.
Returning to Work and Daily Activity
Return-to-work timing depends on hand dominance, the specific procedure, and job demands.
- Office or desk work: 1 to 2 weeks for non-dominant hand surgery. 2 to 4 weeks for dominant hand if the job requires any keyboard or writing use.
- Manual labor or heavy gripping: typically 3 to 4 months, sometimes longer for jobs requiring forceful pinch. Light duty should be arranged.
- Driving: usually 4 to 6 weeks, once out of the cast and with adequate pinch to control the steering wheel.
- Writing, keyboarding, and smartphone use: gradual return over weeks 6 to 12 as part of hand therapy.
Frequently Asked Questions
How do I know if the pain at the base of my thumb is arthritis?
Thumb base arthritis typically causes pain with pinching, gripping, turning a key, or opening a jar. A positive grind test on examination (gentle axial compression and rotation of the thumb reproducing pain) is the classic finding. Standard X-rays confirm the diagnosis and grade the severity of joint space loss. Dr. Loredo evaluates the history, examination, and imaging together to make the diagnosis.
Will a cortisone shot fix thumb arthritis?
Corticosteroid injection into the CMC joint provides meaningful pain relief for many patients and can be repeated over time. It does not reverse the underlying joint wear. When injections no longer hold symptoms at bay, or when injections stop providing relief, surgical reconstruction is the definitive option.
What is the best surgery for thumb arthritis?
Trapeziectomy with ligament reconstruction and tendon interposition (LRTI) is the most established procedure, with decades of good long-term outcomes. Suture suspension arthroplasty is a newer option that avoids harvesting a tendon and may allow faster recovery. Dr. Loredo reviews which procedure best fits your anatomy, hand use, and recovery goals at your evaluation.
How long is recovery from thumb arthritis surgery?
Most patients wear a thumb-protecting splint or cast for 4 to 6 weeks after surgery, followed by hand therapy to restore motion and strength. Light daily activity resumes around week 6. Full recovery with maximum grip and pinch strength typically takes 3 to 6 months, with continued gains for up to a year.
Can I avoid surgery for thumb arthritis?
Many patients manage thumb CMC arthritis for years with a custom thumb spica splint, periodic corticosteroid injections, hand therapy, NSAIDs, and activity modification. Surgery becomes the right option when daily pain persists despite these measures, when the thumb limits activities that matter to you, or when injections stop providing meaningful relief.
When to Call the Doctor
Before treatment, call our office for evaluation if you experience:
- Persistent pain at the base of the thumb with pinching, gripping, or opening jars
- Weakness or dropping objects because the thumb cannot hold a grip
- A visible bump at the base of the thumb that is tender to press
- Grinding or clicking with thumb motion
- Symptoms interfering with work, hobbies, or daily self-care
After surgery, call the office promptly if you experience:
- Fever over 101°F, chills, or flu-like symptoms
- Expanding redness or warmth around the incision or cast
- Thick, yellow, or foul-smelling drainage
- Severe pain that is not controlled by prescribed medication
- Numbness, color change, or loss of motion in the thumb or other fingers
- A cast or splint that feels too tight or has shifted significantly
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- De Quervain's Tendonitis: thumb-side wrist pain from inflamed tendons. Often confused with CMC arthritis because both cause thumb-side pain; the exam and imaging distinguish them.
- Trigger Finger: can affect the thumb (trigger thumb) and coexists with hand arthritis in many patients.
- Carpal Tunnel Syndrome: thumb numbness and weakness from median nerve compression. Different cause, but overlapping symptoms can occur.
- Cubital Tunnel Syndrome: different nerve (ulnar), different fingers (ring and small), but included here for patients presenting with general hand weakness.
- CMC Reconstruction (LRTI / Suspensionplasty): the surgical reconstruction when conservative care has run its course.
From the Blog
- Thumb Arthritis: When Injections Stop Working: how to recognize when cortisone is no longer enough.
- The Basal Joint of the Thumb: why this joint develops arthritis so often.
- CMC Arthroplasty Recovery: realistic 3 to 6 month recovery expectations.
- When a Cortisone Injection Is the Right Choice: early-stage CMC arthritis injection response.
Watch: Thumb arthritis educational videos
Short videos from Dr. Loredo's YouTube and Instagram channels.