Cubital tunnel syndrome is a common condition in which the ulnar nerve is compressed as it passes through the cubital tunnel behind the inner elbow. The condition causes numbness and tingling in the ring and small fingers, weakness of pinch and grip, and in advanced cases visible thinning of the muscles of the hand. Mild cases often improve with night elbow splinting and activity modification. Persistent symptoms are treated with release of the cubital tunnel, which Dr. Loredo performs using an advanced minimally invasive endoscopic technique that returns patients to light daily activity within days.
The Anatomy of the Cubital Tunnel
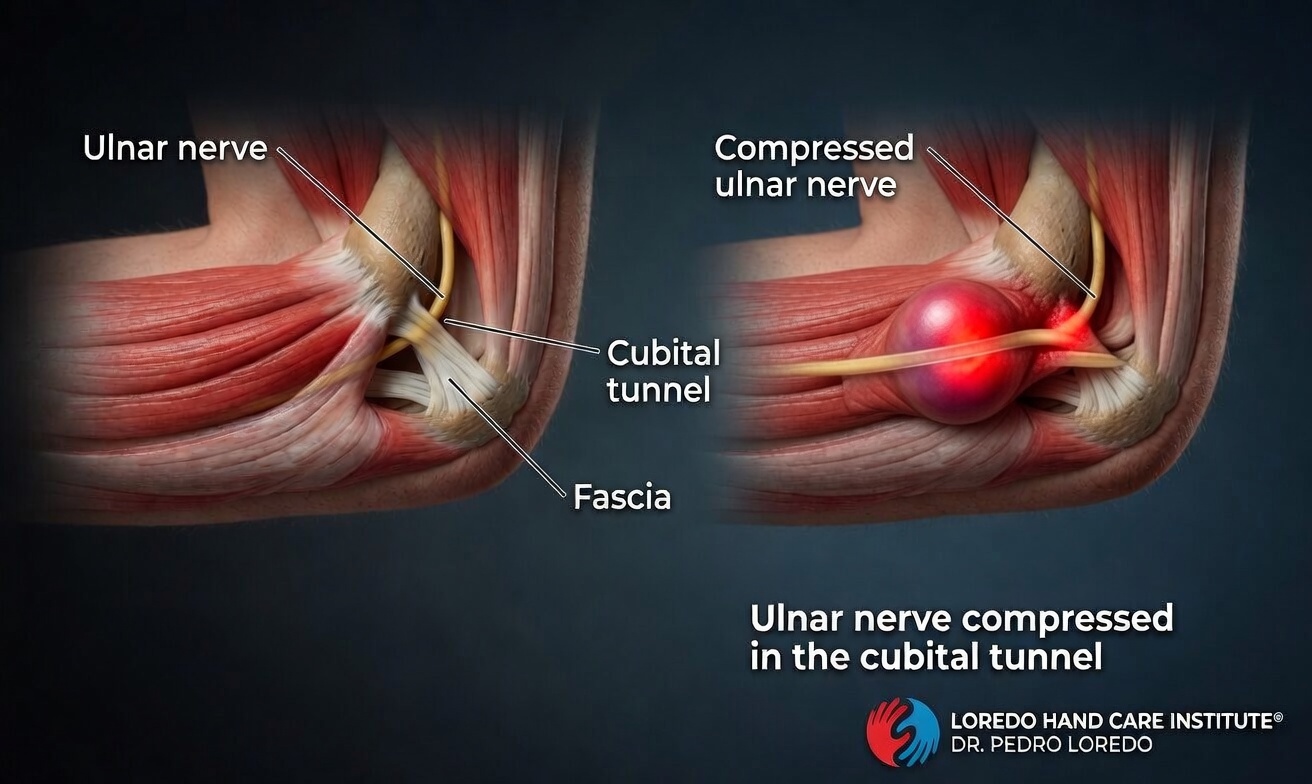
The ulnar nerve runs from the neck down the inside of the upper arm and passes behind the medial epicondyle (the bony bump on the inside of the elbow). At the elbow, the nerve enters a narrow passage called the cubital tunnel, formed by the medial epicondyle, the olecranon, and a fibrous band called Osborne's ligament. Beyond the elbow, the nerve continues down the forearm to supply sensation to the ring and small fingers and motor power to most of the small muscles of the hand. The cubital tunnel narrows further whenever the elbow is bent, which is why prolonged elbow flexion provokes symptoms.
Cubital tunnel syndrome is the second most common peripheral nerve compression in the upper extremity after carpal tunnel syndrome.
Clinical coding: ICD-10 G56.2 (lesion of ulnar nerve). SNOMED CT 85305003 (cubital tunnel syndrome).
Causes and Risk Factors
- Prolonged elbow flexion during sleep, while holding a phone, or at a desk
- Direct pressure on the elbow (resting the elbow on a hard desk edge or car door)
- Repetitive elbow flexion and extension at work or in sports
- Prior elbow fracture, dislocation, or arthritis that changes the shape of the tunnel
- Ulnar nerve subluxation: the nerve snapping over the medial epicondyle with motion
- Diabetes and other systemic conditions that predispose to nerve compression
- Smoking, which reduces blood supply to peripheral nerves
Symptoms and Warning Signs
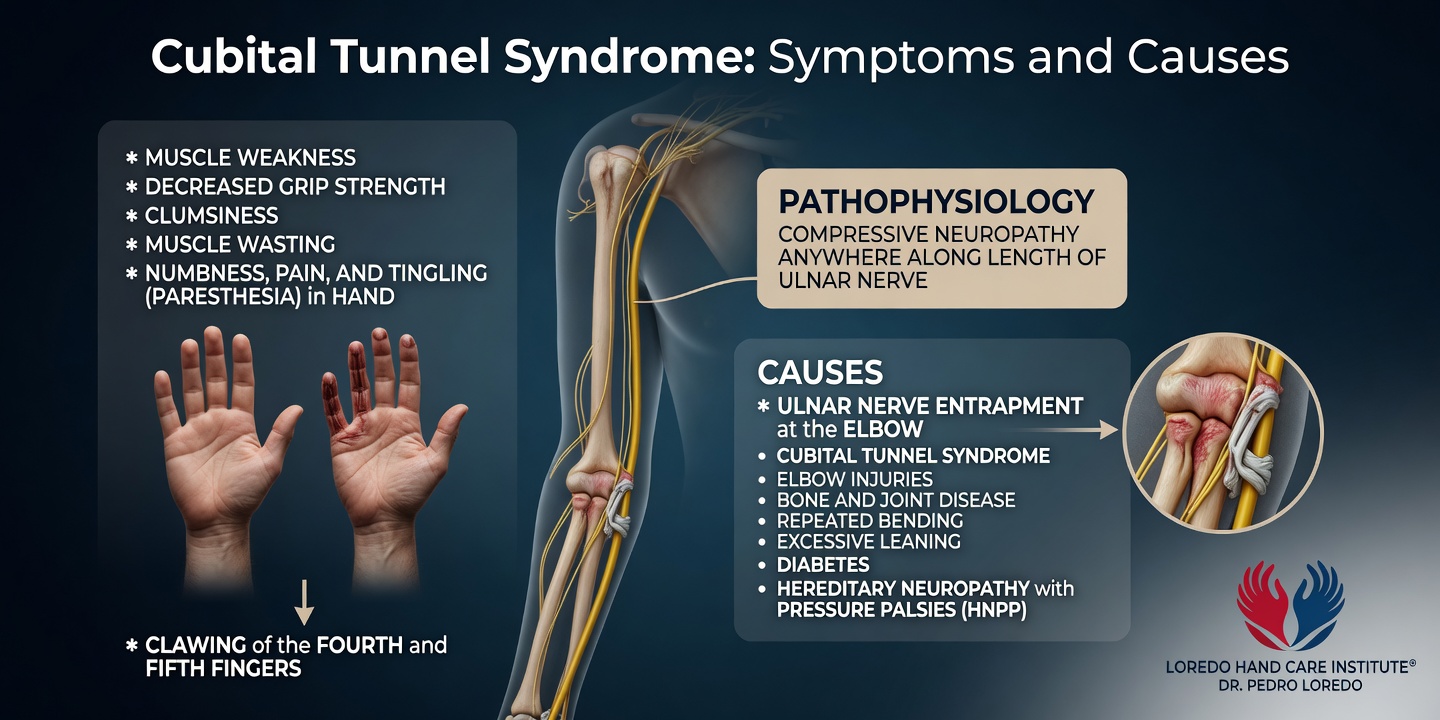
- Numbness and tingling in the ring and small fingers
- Symptoms that worsen with a bent elbow, such as holding a phone or sleeping with the arm flexed
- Elbow pain on the inner side, sometimes radiating into the forearm
- Weakness in pinch and grip, particularly in the small muscles of the hand
- Clumsiness with buttons, coins, and zippers
- A sense that the ring and small fingers cannot spread fully apart
- Visible muscle thinning between the thumb and index finger (the first dorsal interosseous) in severe cases
- Clawing of the ring and small fingers in advanced disease
How the Diagnosis Is Made
Dr. Loredo performs a focused examination including the following provocative tests:
- Tinel sign at the cubital tunnel: tapping over the ulnar nerve behind the medial epicondyle reproduces tingling in the ring and small fingers.
- Elbow flexion test: the elbow is held in maximal flexion for 60 seconds. Reproduction of numbness or tingling is a positive test.
- Froment sign: when the patient pinches a piece of paper between the thumb and index finger, the thumb IP joint flexes excessively if the ulnar-innervated adductor pollicis is weak. A positive sign indicates motor involvement.
- Assessment of the first dorsal interosseous for thinning or weakness.
- Assessment of ulnar nerve subluxation over the medial epicondyle with elbow flexion and extension.
Electrodiagnostic studies (EMG and nerve conduction) confirm the diagnosis, localize the compression, and grade severity. Ultrasound can visualize the nerve at the elbow when the clinical picture is atypical.
Non-Surgical Treatment Options
- Night elbow splinting at approximately 45 degrees of flexion. The splint prevents the prolonged full elbow flexion during sleep that spikes pressure in the cubital tunnel. Often effective alone in mild cases when used consistently.
- Activity modification: avoid prolonged elbow flexion at the desk, in the car, and while holding a phone. Use a headset or speakerphone for long calls.
- Ergonomic adjustment at desk, phone, and car. Avoid resting the elbow on hard surfaces.
- Padded elbow sleeves during the day to cushion the nerve and remind the patient to keep the elbow straighter.
- Hand therapy for nerve gliding exercises.
Conservative care is trialed for 6 to 12 weeks. If symptoms persist, or if muscle thinning or severe numbness is present on initial evaluation, surgical release is recommended.
Surgical Options
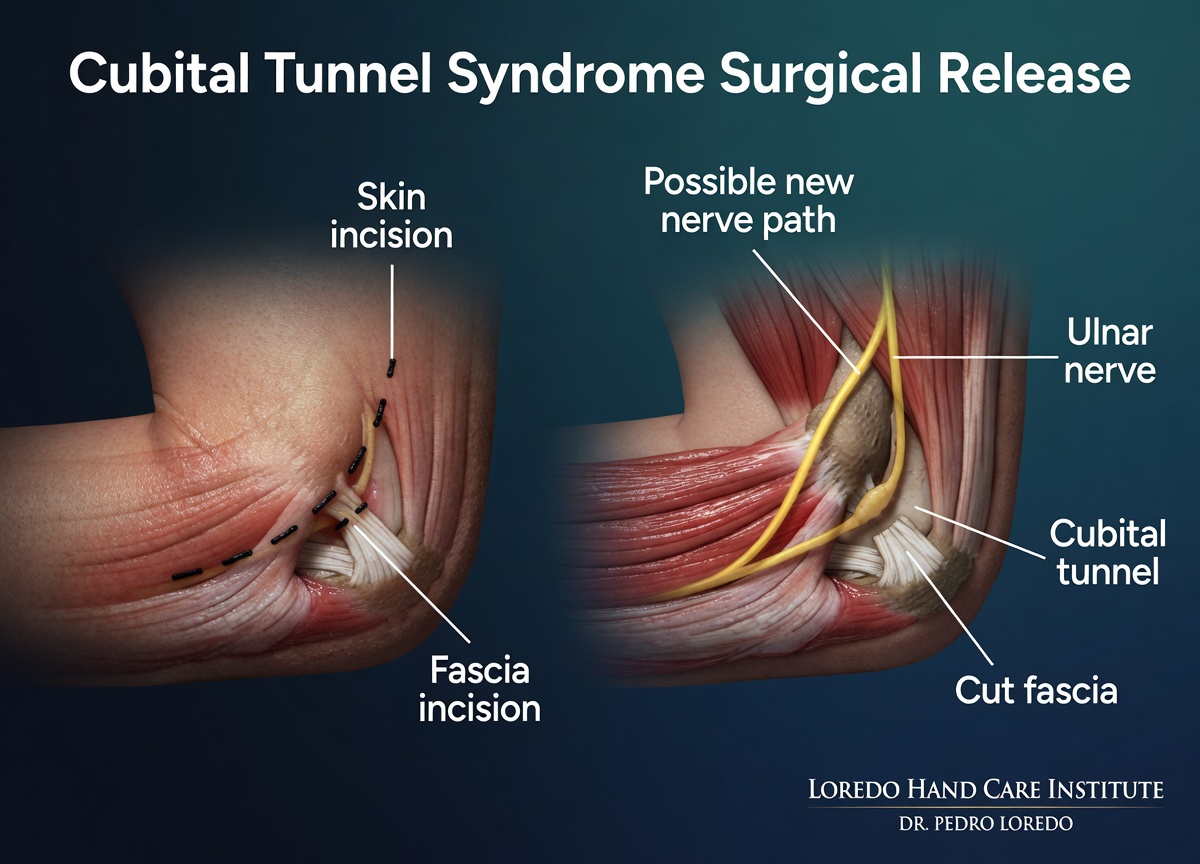
Endoscopic Cubital Tunnel Release (Dr. Loredo's preferred approach)
- Advanced minimally invasive technique under local anesthesia with sedation
- A short incision near the medial epicondyle, with endoscopic visualization of the ulnar nerve
- Complete division of Osborne's ligament and release of the cubital tunnel, with full inspection of the nerve
- The nerve is decompressed in-situ, preserving its natural position
- Rapid return to light daily function within days
Open In-Situ Release
- Traditional approach through a longer incision behind the elbow
- Appropriate for revision surgery or when unusual anatomy is suspected
- Same underlying principle: release the nerve without moving it
Ulnar Nerve Transposition (subcutaneous or submuscular)
- The ulnar nerve is moved from behind the elbow to the front, either under the skin (subcutaneous) or under the flexor-pronator muscle (submuscular)
- Reserved for specific indications: ulnar nerve that subluxates over the medial epicondyle with motion, severe deforming elbow arthritis, or failed prior in-situ release
- Recovery is longer than in-situ release
Most patients do well with in-situ decompression. Dr. Loredo reviews which approach fits your anatomy at your evaluation.
Recovery Timeline
- Day 0: Procedure performed in about 15 to 25 minutes under local anesthesia with light sedation. Soft dressing applied. Gentle finger motion the same day.
- Day 1 to 3: Light hand use for daily activity. Elbow kept comfortable; no heavy lifting on the operated side.
- Week 1 to 2: Desk work typically resumes. First follow-up visit.
- Week 2 to 4: Gentle elbow range-of-motion exercises. Gradual return to driving.
- Week 4 to 6: Return to heavier activity including manual labor, weight training, and athletics, as tolerated.
- Month 2 to 12: Nerve recovery continues, with ongoing improvement in numbness and hand strength. Severe cases take longer.
Returning to Work and Daily Activity
- Office or desk work: 1 to 3 days after endoscopic release. Slightly longer after open or transposition.
- Manual labor or heavy gripping: 4 to 6 weeks. Light duty first if the job requires heavy elbow flexion or vibration.
- Driving: typically within the first week after endoscopic release, once off narcotic medication.
- Exercise and sports: light cardio and lower-body training in week 1. Upper-body strength training after week 4 to 6.
Frequently Asked Questions
Is cubital tunnel syndrome the same as carpal tunnel syndrome?
No. Carpal tunnel is compression of the median nerve at the wrist, causing numbness in the thumb, index, middle, and half of the ring finger. Cubital tunnel is compression of the ulnar nerve at the elbow, causing numbness in the ring and small fingers. Both are common nerve compression conditions in the upper extremity and can sometimes coexist.
Can cubital tunnel syndrome get better without surgery?
Yes. Mild to moderate cases often improve with night elbow splinting, activity modification that limits prolonged elbow flexion, and ergonomic changes. If symptoms have not improved after 6 to 12 weeks of consistent conservative care, or if there is muscle weakness or thinning, surgical release typically becomes the next step.
How long is recovery from cubital tunnel surgery?
After endoscopic cubital tunnel release, most patients resume light daily activity within a few days, return to desk work within 1 to 2 weeks, and return to heavier activity within 4 to 6 weeks. Nerve recovery continues over months in severe cases.
Why should I see a hand surgeon sooner rather than later?
Severe or long-standing ulnar nerve compression carries a higher risk of incomplete recovery. Muscle thinning between the thumb and index finger, persistent numbness in the ring and small fingers, and clumsiness with fine motor tasks are signs of more advanced compression. Earlier surgical release produces the best functional outcomes.
Do I need nerve transposition or just a release?
Most patients do well with in-situ decompression (endoscopic or open release), which leaves the nerve in its natural position. Ulnar nerve transposition, in which the nerve is moved to the front of the elbow, is reserved for specific situations such as the nerve subluxating over the medial epicondyle with elbow motion. Dr. Loredo discusses which approach fits your anatomy at your evaluation.
When to Call the Doctor
Before treatment, call our office for evaluation if you experience:
- Numbness or tingling in the ring and small fingers that wakes you at night
- Trouble with fine motor tasks like buttons, coins, or typing
- A weak grip or difficulty opening jars
- Muscle thinning between the thumb and index finger
- Symptoms that have not improved after 6 weeks of night elbow splinting
After surgery, call the office promptly if you experience:
- Fever over 101°F, chills, or flu-like symptoms
- Expanding redness or warmth around the incision
- Thick, yellow, or foul-smelling drainage from the wound
- Severe pain not controlled by over-the-counter medication
- Numbness that worsens rather than improves
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Carpal Tunnel Syndrome: median nerve compression at the wrist. Different fingers affected, but both are common nerve compressions in the upper extremity and can coexist.
- Trigger Finger: a tendon problem, not a nerve problem. Worth screening if the patient presents with grip weakness plus catching.
- Thumb Basilar Joint Arthritis: a different cause of hand weakness and pain at the base of the thumb.
- De Quervain's Tendonitis: thumb-side wrist pain. Unrelated anatomy, different treatment.
- Endoscopic Cubital Tunnel Release: the surgical procedure that releases Osborne's ligament and decompresses the ulnar nerve.
From the Blog
- Cubital Tunnel Surgery Recovery: day-by-day recovery after endoscopic release.
- Is It Cubital Tunnel or a Pinched Neck Nerve?: distinguishing ulnar nerve from cervical radiculopathy.
- The Ulnar Nerve and Why It Matters: nerve anatomy, Froment sign, and claw hand explained.
- Why Same-Week Hand Surgery Matters: why catching nerve compression early prevents permanent atrophy.
Watch: Cubital tunnel educational videos
Short videos from Dr. Loredo's YouTube and Facebook channels.