De Quervain's tenosynovitis is a painful inflammation of the tendons on the thumb side of the wrist, specifically within the first dorsal compartment. Two tendons (the abductor pollicis longus and the extensor pollicis brevis) run through this compartment, and when their sheath thickens or the tendons swell, movement becomes painful. The condition is especially common in new mothers from repeated infant-lifting, and in anyone who grips or lifts with the thumb repeatedly. Early treatment focuses on thumb spica splinting and corticosteroid injection, which resolves the condition in most first-time cases. When symptoms persist, Dr. Loredo performs a short outpatient release of the first dorsal compartment with most patients back to light activity within days.
The Anatomy of the First Dorsal Compartment
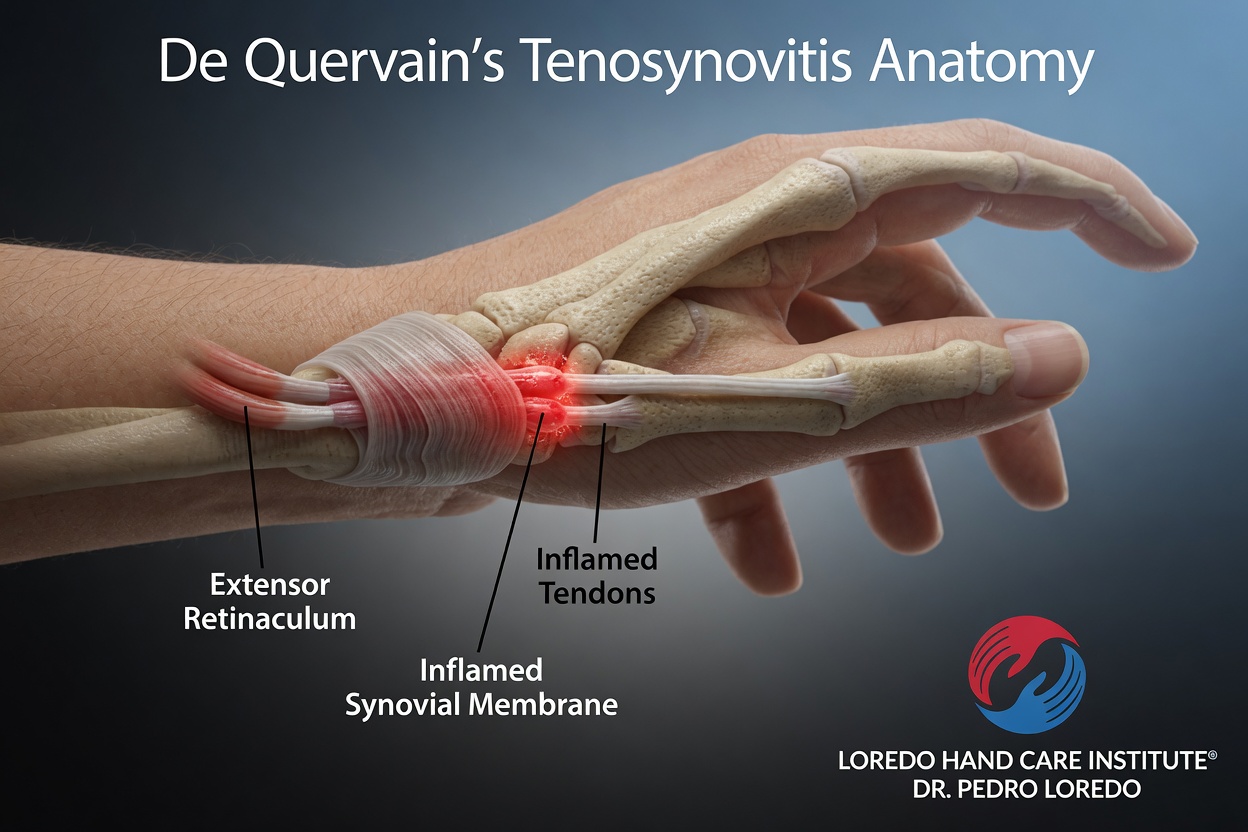
Six tunnels (called dorsal compartments) run across the back of the wrist. The first dorsal compartment sits on the thumb side of the wrist and contains two tendons that move the thumb:
- Abductor pollicis longus (APL): pulls the thumb away from the palm
- Extensor pollicis brevis (EPB): extends the thumb at the MCP joint
In De Quervain's tenosynovitis, the fibrous sheath covering these tendons thickens, or the tendons themselves swell, causing painful friction with every thumb and wrist motion. The condition is especially painful during activities that require both thumb abduction and wrist motion, such as lifting an infant with the thumb extended, wringing out a towel, or using a screwdriver.
Clinical coding: ICD-10 M65.4 (radial styloid tenosynovitis). SNOMED CT 202790007 (De Quervain's disease).
Causes and Risk Factors
- Pregnancy and the postpartum period: the classic "new mother" presentation, from repeated infant-lifting with the thumb abducted. Hormonal changes contribute to tendon sheath swelling.
- Repetitive thumb use: smartphone typing, video game controllers, manual labor involving grip and lift
- Direct wrist trauma that bruises the first dorsal compartment
- Inflammatory conditions: rheumatoid arthritis and psoriatic arthritis
- Female sex: eight to ten times more common in women than men
- Age: most common between 30 and 50
- Diabetes
Symptoms and Warning Signs
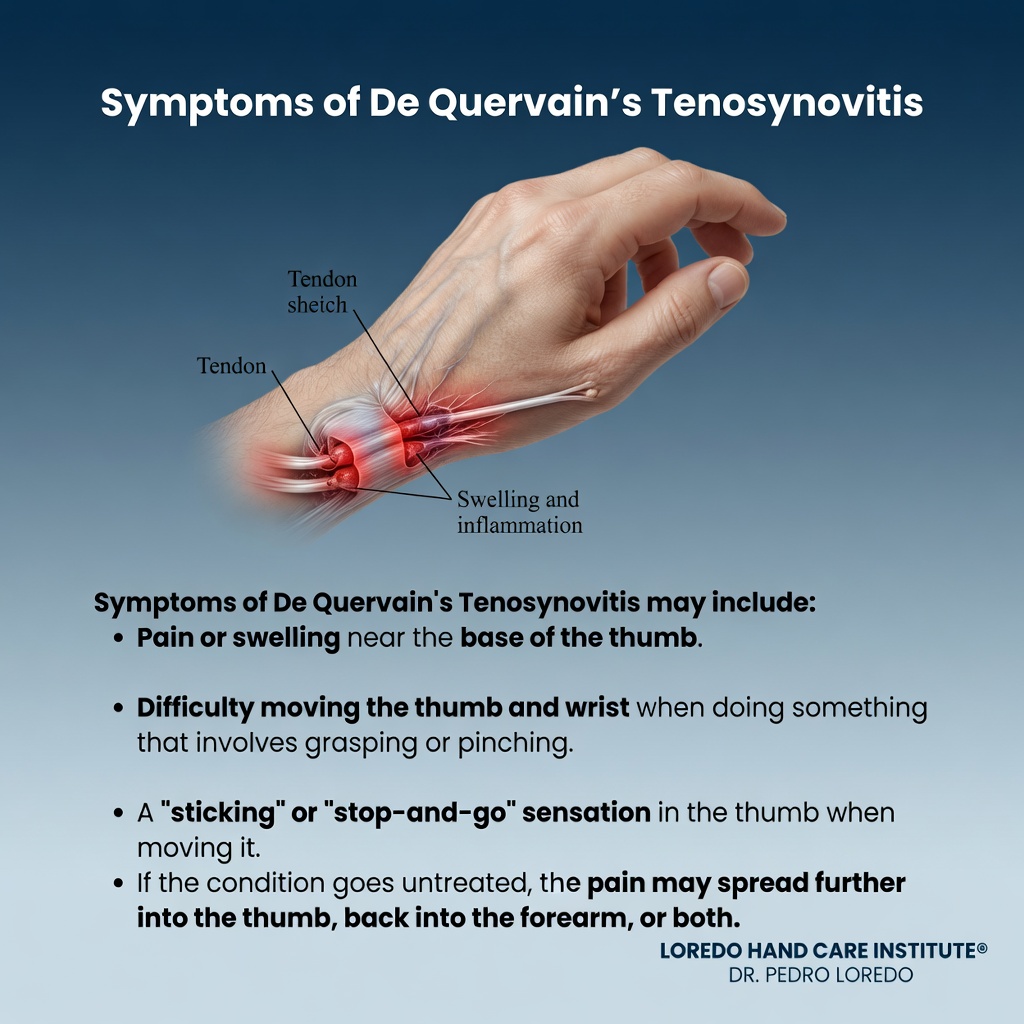
- Pain along the thumb side of the wrist, right over the radial styloid
- Pain worse with thumb-abducted lifting (picking up a baby, a coffee pot, or a casserole dish)
- Pain with wringing, twisting, or opening a jar
- Pain that radiates up the forearm or into the thumb
- Visible swelling or a palpable thickening at the first dorsal compartment
- A feeling of catching or snapping with thumb motion in advanced cases
- Weakness of pinch in long-standing cases
How the Diagnosis Is Made
De Quervain's is a clinical diagnosis. Dr. Loredo's examination includes:
- Finkelstein test (or the Eichhoff variant): the patient tucks the thumb into the palm and the examiner bends the wrist toward the pinky side. Sharp pain over the first dorsal compartment is a positive test.
- Direct palpation of the first dorsal compartment for tenderness, swelling, or a palpable thickening.
- Thumb range of motion and strength testing to exclude other diagnoses.
- Differentiation from CMC arthritis: the grind test should not reproduce the thumb-side wrist pain of De Quervain's. When both conditions coexist, both tests are positive.
Imaging is rarely required. Ultrasound can visualize thickened tendon sheath or a separate EPB sub-compartment when the clinical picture is atypical.
Non-Surgical Treatment Options
- Thumb spica splint immobilizing the thumb and wrist. Rests the tendons and allows inflammation to settle. Worn continuously for 3 to 4 weeks for active cases, then at night and with aggravating activities.
- Activity modification: lift infants with the thumb held close to the hand rather than abducted. Use two hands for lifting. Reduce smartphone thumb use.
- NSAIDs for pain and inflammation (except during breastfeeding without clearance from your obstetrician).
- Corticosteroid injection into the first dorsal compartment. The most effective non-surgical treatment. Resolves symptoms in the majority of first-time cases, with many patients avoiding surgery entirely. Can be repeated once if partial response; three injections are not recommended.
- Targeted hand therapy: tendon gliding, gradual strengthening once pain has subsided, and joint-protection education.

Surgical Options
When corticosteroid injection fails or symptoms recur, surgical release of the first dorsal compartment is the definitive treatment.
First Dorsal Compartment Release
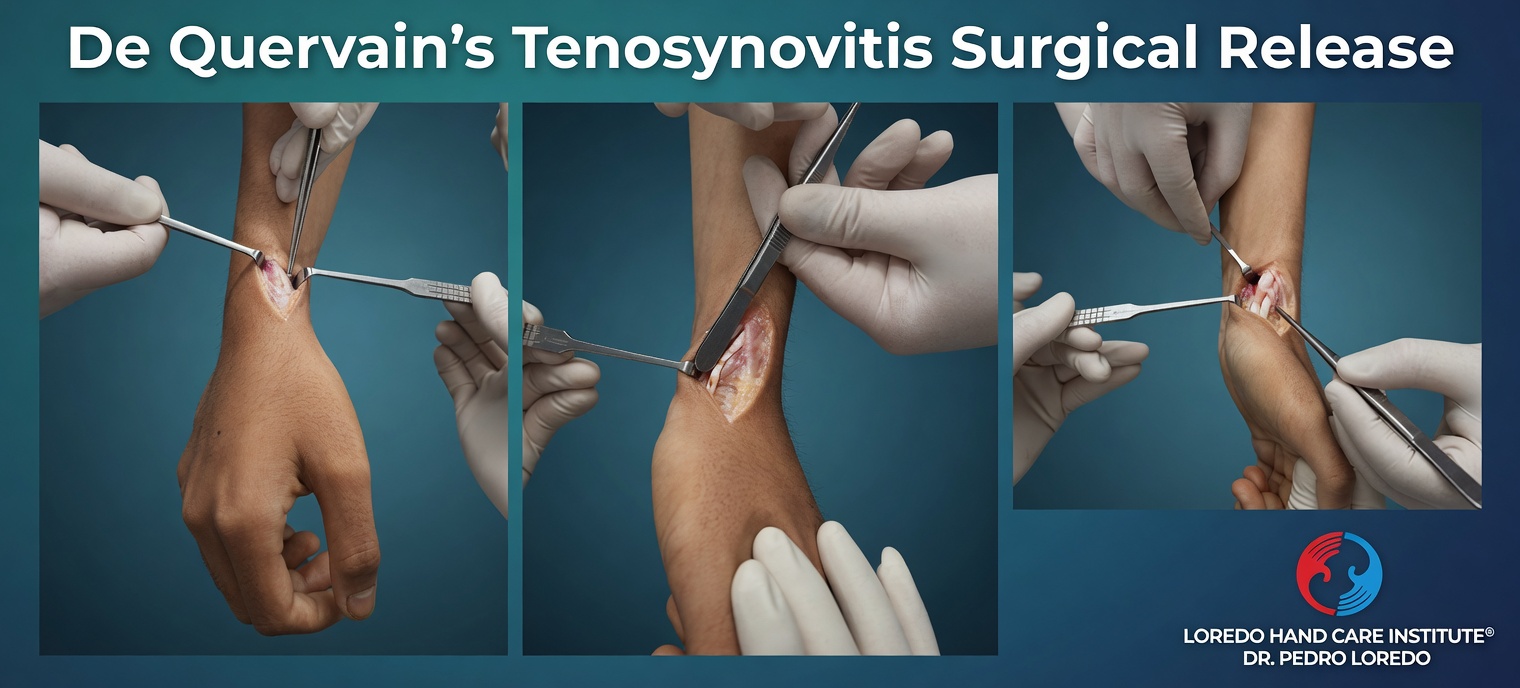
- Short outpatient procedure under local anesthesia
- Small incision over the first dorsal compartment
- Careful division of the fibrous sheath that is compressing the tendons
- Inspection for a separate sub-compartment housing the EPB, which if present must also be released. An unrecognized separate EPB compartment is the main reason De Quervain's release occasionally fails.
- Protection of the superficial radial nerve branches that cross the area
- Procedure time about 10 to 15 minutes
- Light thumb spica splint for comfort for a few days after surgery
Recovery Timeline
- Day 0: Procedure performed in about 10 to 15 minutes under local anesthesia. Light thumb spica splint applied for comfort.
- Day 1 to 3: Light hand use. Splint worn for comfort, removed for gentle motion.
- Week 1: Splint typically discontinued. Most patients back to desk work.
- Week 2 to 4: Return to daily gripping and lifting activities.
- Week 4 to 6: Return to manual labor, athletics, and heavy tool use as tolerated.
- Week 6 to 12: Scar softens. Residual tenderness at the incision resolves.
After a successful corticosteroid injection, the recovery is shorter: pain improves over 1 to 2 weeks, and most patients are back to all activities within 2 to 4 weeks of the injection.
Returning to Work and Daily Activity
- Office or desk work: 2 to 3 days after surgical release
- Manual labor or heavy gripping: 4 to 6 weeks. Light duty first if the job involves sustained thumb-abducted lifting.
- Driving: usually within the first week after surgery once pain-free grip is restored
- Infant-lifting for new mothers: gradual return with technique education in week 1 to 2. Keep the thumb close to the hand, lift from the trunk, and use both hands when possible.
- Smartphone and keyboard use: light use immediately after surgery; full use within a week.
Frequently Asked Questions
Is De Quervain's common during pregnancy and after delivery?
Yes. De Quervain's tenosynovitis often begins in the third trimester or the postpartum period. Repeated infant-lifting with the thumb abducted is a major contributor. Many cases improve with thumb spica splinting and modified lifting technique, though some require corticosteroid injection or surgical release when persistent.
Is a cortisone injection effective for De Quervain's?
Corticosteroid injection into the first dorsal compartment resolves symptoms in the majority of first-time cases. Many patients avoid surgery entirely with one well-placed injection. When symptoms recur after two injections or response is incomplete, surgical release of the first dorsal compartment is the definitive treatment.
How do I know if it is De Quervain's or CMC arthritis?
Both conditions cause thumb-side pain but in different locations. De Quervain's pain is at the first dorsal compartment on the back of the thumb side of the wrist and worsens with a positive Finkelstein test. CMC arthritis pain is at the base of the thumb itself and worsens with the grind test. Dr. Loredo's examination plus X-rays when needed distinguishes the two.
How fast is recovery from De Quervain's release surgery?
The procedure takes about 10 to 15 minutes under local anesthesia. Most patients use the hand lightly within days, return to desk work in 2 to 3 days, and resume heavier activity within 4 to 6 weeks. A light thumb spica splint is worn briefly after surgery for comfort.
Can De Quervain's come back after treatment?
Recurrence after complete surgical release is uncommon. When symptoms persist or return, the most likely causes are a separate tendon compartment within the first dorsal compartment that was not fully released, scar tissue, or a different diagnosis such as intersection syndrome or CMC arthritis. A fellowship-trained hand surgeon can evaluate the specific pattern.
When to Call the Doctor
Before treatment, call our office for evaluation if you experience:
- Thumb-side wrist pain that worsens with lifting or wringing
- Pain that interferes with caring for a baby, working at a keyboard, or using tools
- Visible swelling or a tender bump at the thumb-side wrist
- Symptoms that have not improved after 4 to 6 weeks of splinting
- New pain in a postpartum patient
After surgery, call the office promptly if you experience:
- Fever over 101°F, chills, or flu-like symptoms
- Expanding redness or warmth around the incision
- Thick, yellow, or foul-smelling drainage from the wound
- Severe pain that is not controlled by over-the-counter medication
- Numbness on the back of the thumb or index finger (possible superficial radial nerve issue)
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Thumb Basilar Joint Arthritis: thumb-base pain from joint wear. Often confused with De Quervain's; can coexist. The grind test versus Finkelstein test distinguishes them.
- Trigger Finger: a tendon problem in a different location (A1 pulley in the palm). Can involve the thumb (trigger thumb).
- Carpal Tunnel Syndrome: thumb numbness from nerve compression; different cause but both common in pregnancy and postpartum.
- Cubital Tunnel Syndrome: an unrelated nerve compression, included for patients presenting with general hand and wrist symptoms.
- De Quervain's Release: the definitive surgical procedure when injection and splinting fail.
From the Blog
- De Quervain Release Recovery Guide: bandage care, suture removal, scar management, return to baby holding.
- Intersection Syndrome vs De Quervain: two wrist tendinopathies that look similar but are anatomically distinct.
- When a Cortisone Injection Is the Right Choice: expected response and duration of relief.
Watch: De Quervain's educational videos
Short videos from Dr. Loredo's Instagram and Facebook channels.